 A new model to explain rhythmic phenomena observed during Craniosacral therapy
A new model to explain rhythmic phenomena observed during Craniosacral therapy
A new model to explain rhythmic phenomena observed during Craniosacral therapy
A new model to explain rhythmic phenomena observed during Craniosacral therapy
(PS - I don't agree with much of this model now (May 2012), but the description of the Monroe-Kelly Doctrine with balloons is still valid, and the whole is still an interesting read, food for thought, and still contains some useful material. The 10-second CRI is the most "physical" of the Cranial rhythms, and its physicality suggests a fairly physical and potentially identifiable origin. The two main physical mechanisms that I currently consider relevant are a) vascular volume changes mainly in the VENOUS system (cavernous sinuses and the venous plexus in the vertebral canal), and b) osmotic forces due to periodic variations in dissolved Oxygen, resulting from a resonance between cardiac pulse, the respiratory cycle and the krebs cycle, probably playing out quite strongly in the capilliary bodies. The science behind the production and reabsorption of flow of CSF has also moved on since I wrote this. For more up-to-date conceptual models, see the Professional resources page - especially the Swedenborg/Pollack papers.
The Craniosacral rhythm (CSR) can be felt throughout the whole body by trained hands, and has been proven to exist by a wide range of different studies (e.g. see CSTA) ). This paper presents a new physiological basis for the CSR, which also explains many other healing phenonena. Arteries naturally resonate due to chaotic turbulence at the arterial branching. This resonance "sounds" throughout the arterial system, and resonant beats occur at various frequencies, including very long beats at several cycles per minute. Arterial dilation squeezes the Craniosacral fluid, creating the phenomenon of the CSR. There is a three-way feedback between the sympathetic nervous sytsem, the arterial resonance pattern, and the Craniosacral rhythm.
| CSR | Craniosacral rhythm |
| CSF | Cerebro-Spinal Fluid |
| CSS | Cranio-Sacral System (the Dura, everything contained with it, and the bones on the outside of it) |
| cpm | cycles per minute |
| Hz | Hertz (cycles per second) |
| CV4 | Compression of the 4th Ventricle - a specific Cranial technique |
This short article looks at a simple model for observed rhythmic behaviour of the physiological CSR, which
I have written an introduction to the fluid mechanics of the CSS, because it is relevant to the detailed functioning of the proposed model.
For Craniosacral Therapists reading this paper, I ask that you temporarily unlink in your mind the two concepts of CSF production and CSR - and allow them to have the possibility somewhat different driving mechanisms.
The Craniosacral Rhythm (CSR) is a phenomenon which has been described by several authors (e.g. Upledger), and which can be felt by a trained pair of hands, or detected by strain gauge/radio interferometry techniques on living mammals (I've never tried to feel the CSR of a frog!). The CSR appears to operate over several discrete frequency ranges. The fastest recognised CSR (about 30 cpm) is pathological, and is associated with disrupted nerve connection (as in the case of paraplegia). In health, the commonly recognised baseline CSR lies between 5 and 12 cpm. Much slower rhythms (less than 2cpm) have been found by observers, which coincide with self-induced deep states of relaxation and dream-like synaesthetic internal awareness. The CSR may also enter a "stillpoint", which is characterised by a reduction in total electrical activity in the body, and internal physiological changes which often result in a reduction in muscle tension and pain.
The skull accomodates the pressure changes during the CSR by changing shape. It becomes more round as pressure increases ("Flexion"), and becomes more narrow and elongated as pressure decreases ("Extension"). For more information on the Craniosacral system, see CST Links page.
If you don't feel technical, are impatient, or are happy with fluid-elastic hydraulics, the guts of the paper starts at section 3 (although the following contains some interesting ideas which are worth looking at...)
This is a review of the mechanical properties of fluid-filled elastic systems. The connective tissue network of the body is highly complex, and has a range of different properties which make it particularly special. Elasticity is only one of these properties, and fills an important role in the Tensegrity of the body, down to a sub-cellular level. Another property of the connective tissue system is its semiconducting nature- which clearly indicates a potential for electrical and electromagnetic effects within living organisms.
As a fluid-filled elastic balloon, the human body has an internal pressure of shape, and internal pressure differentials between membranous compartments (e.g. between the CSS and vascular systems). The ability of these compartments to respond to (and allow) volume transfers is dependent on their leakiness (i.e. how much throughput is possible), and their relative elasticity. For example, If you have a thick rubber tyre and a thin toy balloon connected together, the tyre will change volume by a relatively small amount as its internal pressure is increased, whereas the thin balloon will expand massively under the same pressure. If you take this underwater, the tyre will again virtually remain unchanged, but the balloon will now be strongly invaginated into the tyre. A tiny hole in the balloon (or tyre) if they contained air (and were placed in air) would result in a gradual movement towards equilibrium with the surrounding air.
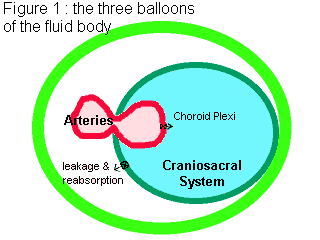
The Craniosacral fluid system is essentially an elastic balloon filled with salty water, and large concentrations of neurotransmitters. The dura and the vascular sleeves are particularly strong elastic - like car tyres - and so are not particularly good at absorbing volume. When they suddenly absorb an additional volume, their tendency is to quickly force it out again - due to the increased pressure caused by the elastic membrane expansion - or to bellow out at their thinnest point (hence aneurysms). The thin rubber balloon is the remainder of the body.
The elastic pressured systems we are culturally most familiar with are AIR-filled, such as tyres, air beds, swimming aids and toy balloons. Whilst some principles are the same, there are substantial differences in behaviour between air and fluid-filled balloons to warrant some discussion. For best understanding, take two balloons. Fill one with air and tie the end up. Fill the other with water, and hold it tightly to stop the water escaping.
Firstly, the air-filed balloon. Feel the rubber membrane - notice how tight it has become as it stretches to meet the pressure of the air inside. Also notice how the stretch is equal over the whole area of the balloon surface. The degree of stretch is related to the following factors :
When the balloon stretches, it also squeezes whatever is inside it (simple experiment - stretch an elastic band round your finger - as you stretch it more, it squeezes more). This elastic squeeze is equal to the pressure difference between the pressure of inside filling (air or water) and the outside pressure.
Now, if you squeeze the air filled balloon, you will notice that it does not easily change volume. This is because the air inside compresses far more than the elastic stretches, and so pressure changes are absorbed as much by the air as the elasticity of the balloon. Similarly, if you blow into the balloon, the air you put in is compressed, and so volume going in is NOT the same as volume change in the balloon.
Elastic systems tend to become more spherical as their internal pressure increases, because this is the most efficient expression of the balance between volume and elastic expansion. Mathematically, spheres have the greatest volume to surface area ratio of all 3D shapes. In a similar way, the skull is slightly more spherical at the end of the flexion phase of the CSR. It achieves this by small movements of the Cranial bones, which articulate against each other, and bend. (Incidentally, the usual image of bones is as hard, almost lifeless rigid bars and plates. Living bones are flexible, exhibit piezoluminescent effects - they emit flashes of light when they are stressed - and are filled with blood vessels and nerves.)
As a final experiment with the air filled balloon, select some music with a fairly heavy drum beat, and stand holding the balloon in front of your HiFi speakers. What do you feel in your hands?
If we consider the water filled balloon, then it can have several surprises. Firstly, hold it by the spout, tightly so that water cannot come out. Now with the spout pointing upwards, slowly release the hold with your fingers until the water starts to come out (do this over a sink!). If this was air, the volume coming out would be mainly due to expanding air (say you blow into a balloon, and then let the air come back into your mouth!) For water, the pressure which sends the water spurting upwards is purely due to the elasticity of the balloon squeezing the water. Water-filled systems respond much more quickly than gas-filled ones. The tiniest droplet of fluid leaking from a non-elastic container would equalise the internal and external pressures, whereas air would take a long time to decompress. Water can be compressed, but only by about 1 part in 10 million per metre of water pressure. This compressibility is important for transmitting sound and vibration, but obviously unrelated to the behaviour of the water squirting up into the air. Now refill the balloon with water, allow the air to be pushed out, and then tie the end of the balloon. You now have a model of the Craniosacral system - accurate with the following exceptions :
However, we can still learn something more about the behaviour of the CSS by squeezing one end of the balloon. The other end immediately expands, and the fluid inside the balloon shifts its position. Your hand has relieved the elastic tension in the balloon it is squeezing, and so this is compensated by an increase in tension in the remainder of the balloon. The area of balloon expanding is less than the whole of the balloon, and so the pressure (and elastic stretch) on the unsqueezed balloon is increased. Water is at a higher pressure, BUT it still occupies the same volume. The increased pressure on (and in!) the water comes purely from the increased elastic stretch in the balloon. Another way of looking at this is to recognise that the balloon is now less spherical, and so (from a purely geometrical point of view) must stretch more wherever it can in order to contain the same volume of fluid.
One interesting fact about a contained fluid is that it exerts equal pressure in ALL directions. For a balloon, this means that it stretches equally over all of its area. Consider the fact that the CSS is contained at its base by the spinal canal. It will naturally exert a substantial expansive force on the spine - mainly outwards and equally on all vertebrae, but also longitudinally (up and down), encouraging the spine to remain as long as possible. You might even say that the function of the vertebrae is to contain this fluid, and the spine will remain upright simply because it is filled with slightly pressurised fluid. The spine can now be seen as a Tensegrity structure with a fluid core - and muscles are only required to move it (rather than support it). If you do need muscles to support your spine, it is only because they are pulling against other (tight) muscles or against unusually tense connective tissue. This is one reason why your spine is able to re-lengthen at night, and the CSR encourages this lengthening by internal traction and movement. Try measuring your height immediately before you go to bed, and immediately after you get up in the morning.
The other point to note is that if fluid only ever entered and left within this upper part of the balloon, the area in your hand - equivalent to the volume of fluid in the spinal canal - would inevitably stagnate. The pumping action of the CSR itself will encourage a small degree of mixing - as happens within a tidal inlet - but the waters in a inlet take a very very long time to move into the more dynamic ocean, and are usually far more saline and muddy. I infer from this that there must be some outlets for the CSF along the spine - at least in the sacral area. Alternatively, fluid passes down the spine in (say) the central canal of the spinal cord, and back up again through the subarachnoid space. With my present anatomical knowledge, I find this second (more orthodox) model unbelievable, despite the arrows shown in Netter [11], plate 103. The lateral and median apertures of the 4th ventricle equalise the pressure between the ventricles and the arachnoid space, and so there is no pressure gradient available to create contradirectional flow within the spinal canal.
If we think about posible sources and exits for the CSF, its source must be arterial blood. This is the highest pressured fluid in the body, and fluid enters the CSS from arterial blood filtered through the choroid plexi. The CSF exits to the venous system (via the arachnoid villi), and to the fluids in the body cavity via the Cranial and spinal nerve roots. In saying this, I have automatically assumed one of the fundamental laws of fluid flow - namely that flow is ALWAYS from high pressure to low pressure.
There are no holes in the body which allow fluid to move between the CSS and the remainder of the body. Yes - there are holes within the CSS which allow flow between different chambers of the CSS, but flow into and out of the CSS is through semi-permeable biological membranes, which filter the fluid and provide an immune barrier. The semipermeable nature of these membranes creates additional sources of pressure relative to external fluid systems, which affects the movement of fluid in and out of the CSS, through the mechanisms of coupled chemical, thermal (and electrical!) diffusion. If there is a chemical or thermal gradient across a semipermeable membrane, this naturally causes a pressure differential to be established. This is one reason why deep (1000 metres down or more) enclosed pockets of water can be found in the earth at a massively different pressure than they "ought" to be, given their geological setting. The semipermeable membrane (of clay, for instance), creates a thermal and chemical pressure gradient which can be many times the fluid pressure due to normal containment. Pressure decreases towards the lowest temperature, and towards the highest saline concentration (very roughly speaking - the exact osmotic potential is dependent on the exact proportions of dissolved solids). Since core body temperature is slightly higher than temperature at extremities, thermal diffusion will tend to favour flow out of the CSS. Similarly, I understand that the salinity of the CSS is less than that of the blood, and so again this will favour flow out of the CSS back into the venous system.
Electrical potentials also create a differential pressure across a semipermeable membrane. We know that body surface potential varies by about 20mv down the spine (see Cade and Coxhead, or try it for yourself by using a multimeter - you have to measure quickly and use strong saline solution on the skin. If you take more than a few seconds to get the reading, your body will compensate and change the potential across the multimeter to zero!), so internal pressure potentials may be substantially larger as a result of electrical activity.
Flow into and out of the CSS is dependent on these factors of hydraulic pressure difference, thermal gradients, electrical potential, and osmotic potential. The CSS internal pressure must always lie somewhere between the two extremes of the systems supplying and receiving flow, allowing for all these additional sources of pressure.
Now, consider flow entering and leaving this balloon of the CSS. If the flow entering is greater than the flow leaving, then the volume inside increases, and so the balloon MUST expand. When it expands, it becomes more stretched, and so pressure increases. Therefore, as the volume of fluid in the CSS increases, the pressure inside the CSS also increases due to elastic expansion. The very nature of a system of water enclosed by elastic means that :
Dynamic systems with relatively high velocity flows (e.g. blood) themselves have an internal pressure differential if there is even the slightest resistance to flow. This is because flow is turbulent rather than laminar, and so friction losses are large. (Also, turbulent flow is well mixed, which is practically of great importance to blood). For example, the pressure at your mains supply will always be greater than the pressure at a flowing tap, because the flow itself absorbs pressure (friction losses). However, the pressure of water in the tap is greater than that of the surrounding air, and so the water can flow out of the tap. If you connect a short pipe between hot and cold taps, and turn them both on, then the water will flow towards the lowest pressure system - usually cold water will flow into the hot water pipes. When you close the tap, the pressure inside returns to the same pressure as the mains water supply, because zero flow means zero friction losses. The pressure difference between venous and arterial systems is essentially a measure of the amount of resuistance to flow which must be overcome to transmit this quantity of blood.
The total volume of CSF is about 120 to 150cc, and it is replaced "several times every day", inferring a total flow of less than 1 litre per day, or less than 0.7cc/minute. Therefore, even in the restricted space of the central vertebral canal, relatively low velocities will be present, flow will tend to be laminar. This means internal pressure gradients can be quite small, and mixing will tend to be through the pulsing motion of the CSR and internal diffusion. (Caveat - I make this statement with no access to Reynolds Number data for the CSF. It may be that the CSF is sufficiently viscous to create turbulence even in the ventricles. This makes more physiological sense, because it allows far easier mixing of neurotransmitters.) Taking the extreme case of hydrocephalus, the excess pressure in the head is not necessarily caused by a total blockage of the CSF, but may instead be the overpressure required to maintain flow (to wherever the outflow point is) against restriction.
The pressurestat model is supposed to give a physiologically based description of CSF generation in the brain and possibly spinal chord. Its mechanism is based on the idea that stretch receptors in the sagittal suture reduce and increase inflow of CSF as normal limits of motion are attained. The CSR is seen to be directly caused by step changes in CSF production. So far, I've been unhappy with this model, because it does not adequately describe phenomena observed in the CSS (see below). One question I would raise is, given the previous discussion of the necessity of pressure gradients to fluid flow, why does the CSR not respond to blood pressure changes in the arterial system (pulse)? If the CSR is truly caused by production of fluid at the choroid plexus, then surely we would feel the pulse of arterial pressure - even if this pulse is too rapid to cause elastic system compliance? I partly have an answer to this, in that the double bend on the Carotid Artery as it enters the cranium may act as a pressure regulator, dampening peak pressure surges. It may also set up some very interesting resonances within the local blood vessels. Nevertheless ....
When looked at from the point of view of the pressurestat model, I have experienced some unaccountable CSR behaviour, including
There is no doubt that cells resonate, both electrically and physically, and that resonance is entrained by driving frequencies in the body, and in the electrical environment of the Earth. The cell resonance model is based on the assumption that the CSR is caused by interference patterns between cells with similar respiration frequencies - e.g. the Glial cells, or even the cells of the entire body.
Low frequency beats are caused by two similar higher frequency waves - e.g. a 0.1 Hz wave (i.e. 10 seconds per cycle or 6cpm) could be generated by interference between two waveforms of mutually similar amplitude, and frequencies of (say) 10.0 and 10.1 Hz. I've tried playing around with different sine waves to create an interference pattern similar to the CSR (Figure 2), but if cellular resonance is the cause of BOTH the CSR and the throughflow of CSF, it would have to exert substantial force in order to display the phenomena associated with the CSS. I recognise that there are vibrational patterns at a fundamental cellular level, but it seems that something more physically powerful is required to produce the physiological effects...
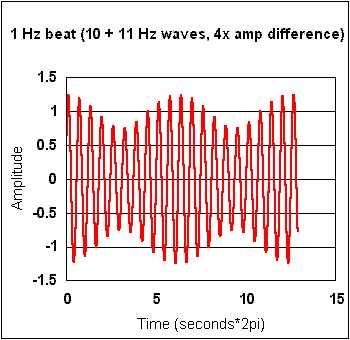
FIGURE 2 : TWO SIGNALS (10Hz and 10.1Hz) COMBINE TO CREATE A 10Hz BEAT
A substantial amount of evidence exists from blood pressure research (see refs 1-9) to indicate that the body has a periodic expansion and contraction, lying in between the diurnal (daily) cycles and the cardiac pulse (heartbeat). This sub-Hertzian rhythm may be the same rhythm observed in cranial fluid motion. Furthermore, dilations of arteries and veins due to these long rhythms have been measured, and shown to be sometimes greater than the dilations caused by the cardiac pulse! The measured pulsations appear to be caused by chaotic resonance within the vascular system. Fluid turbulence at branchings (i.e. nodes at which the flow diverges in arteries), causes each length of artery to resonate, rather like an organ pipe. All of these resonances in turn resonate throughout the entire arterial fluid system, and so a complex multifrequency system of beats is produced. This resonance pattern is itself dependent on sympathetic tone of the arterial smooth muscle, and simultaneously apears to feed back into the tonus of the arterial walls. It has been proposed that there may be a distributed control system (at the arterial branchings) which feeds back into a central resonance pattern. This resonance is one of the mechanisms by which the body controls blood pressure - especially in emergency situations. I suggest that a similar resonance pattern also exists in veins due to turbulence at converging nodes, although this has not been measured as yet (blood pressure research tends to focus on arteries).
The above research suggests that the CSR may be a "ballon within a balloon" response to a physiological rhythm (chaotic resonance) in the arteries.
Briefly,
The direction of flow during flexion and extension would be the reverse of the pressurestat model. CSF is produced at a fairly regular rate, which decreases during flexion, and increases during extension. This cyclic change in CSF production is due to changing pressure differentials between the CSS and the arterial system - as internal CSS pressure increases, inflow to the system decreases.
The mobility of the Cranial bones is determined by the balance between dural elasticity and the elastic resilience of the external systems in contact with the CSS. Low mobility would be due to decreased dural elasticity, or decreased elasticity of arteries (in which case the arteries in the body cavity outside the spine would accomodate some of the pressure/volume change.
A puncture to the system would apparently demonstrate increased fluid production during flexion. This is an illusion caused by fluid displacement by the expanding arterial walls. Also, a puncture would not disrupt the CSR, since the CSR is not strongly coupled to CSF. This ties in well with observed reactions to brain surgery and lumbar punctures, but may also have led to incorrect assumptions regarding daily CSF production - I would be very interested in seeing original research protocols for measuring CSF flow to check this out.
I finally suggest that the sensation of flow experienced during CSS palpation - including off-body sensations of movement - are at least partly caused by the movement of the physical resonance pattern within the arterial system. I strongly suspect that there is a mechanism for conversion or communication between physical vibration and electromagnetic frequency phenomena in living systems. This may be held at cell level, but one possible large scale visceral location of this vibratory-EM transduction is given later.
This proposed mechanism for the CSR (namely arterial resonance) allows a simple explanation of much of the behaviour which the Craniosacral motion exhibits which do not easily fit into the presurestat model. Variations in CSR - including stillpoints - may therefore be due to chaotic shifts in this vascular resonance.
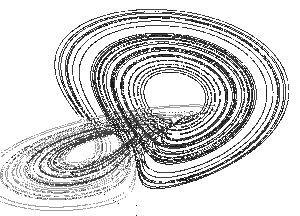
Because the arterial resonance system is chaotic, it would tend to follow a strange attractor pattern, holding to one resonance range, and then suddenly dropping down to a lower resonance frequency. Figure 3 shows a Lorenz attractor in a caotic system - despite the apparent chaos, there is an order of sorts - in fact, a rather beautiful one. This is in direct contradiction to the second law of thermodynamics, and has been explored by Murray Gell-Mann in his book "The Quark and the Jaguar".
There is a direct analogy in global weather patterns. The system will accomodate changes in environment as much as possible, whilst staying in the same chaotic attractor pattern, before suddenly jumping to a different chaotic attractor pattern which enables a certain stability to be maintained under the (previously) extreme conditions. This is a possible mechanism for the sudden "thuds" which are felt in the CSR immediately prior to some stillpoints, as the resonance pattern suddenly ("catastrohically") shifts to a different (stable) pattern. Of course, a sudden local convergence of resonant patterns would also explain this phenomenon
Chaotic systems have the properties of being particularly stable within a (homoeostatic) range, easily controlled by feedback mechanisms, and very sensitive to tiny local changes. This makes them ideal for biological systems, and chaotic behaviour is found throughout the natural world. For some more thoughts on chaos and health, see Nigel Hargreaves. Pacemakers are now fitted with a chaotic beat generator, because a totally regular beat was found to be poorly accepted by the body. I suspect that the broad range frequencies of the arterial chaotic resonance system can account for various therapeutic methods, including :
The sensitivity of chaotic systems is captured in the well known image of a butterflies wing beat in Beijing creating a storm in New York. It is possible to see how a therapist in body contact with a person can make changes and cause therapeutic pulsing to occur (and how sometimes healers pick up symptoms from their clients). An entrainment process occurs between the two people, and resonant patterns develop in both their bodies. Hence the ambiguity of where a therapeutic pulse is coming from - is it my hand/body or theirs? Probably both, and it probably doesn't matter. In some senses, this does matter, of course, because of the problem of transfer of pathology to healers. I used to experience a lot more problems with this - and have had virtually no difficulty over the past two years. Factors which appear to have helped are :
Returning to the subject of resonant patterns, research in China has shown that Chi healing includes the phenomenon of sub-sonic sound emissions from the healers palm. These occur as chaotic frequency patterns falling between 7 and 14Hz. It now becomes quite easy to see (at least in outline!) how this form of healing works - the subsonic emissions are probably due to arterial resonance, and they in turn pass deep into the body and entrain local resonance patterns. Similar comments have been made by Yogis - namely that a kundalini rising is preceded by aortic resonance at about 7Hz [14]. The link between EM and vibrational activity on the body is further underlined by the research of Zimmerman [13], which found pulsed EM fields in the range 0.3 to 30Hz (mainly around 7 to 8Hz) around a healers hands. This series of coincidences also clearly underlines the link between biological frequencies and environmental frequencies (in this case, the dominant Schuman frequency). It is perhaps relevant to point out that the EM frequency ranges correlated by Valerie Hunt with regards to Chakra activity (i.e. about 10kHz to 500kHz) lie within the frequency range most favoured by research into natural sources of free energy.
There are many driving frequencies in the environment. The most well known are the diurnal and lunar cycles, but longer cycles exist - such as sunspot cycles of 11.2 years, and shorter cycles such as Schuman resonances (7.83Hz and beyond), and magnetospheric resonance (Figure 4). There is even an electromagnetic resonance in the solar wind due to a bow wave effect on the magetospheres of all the planets in the solar system, and this resonance lies in the range 1 - 3 Hz.
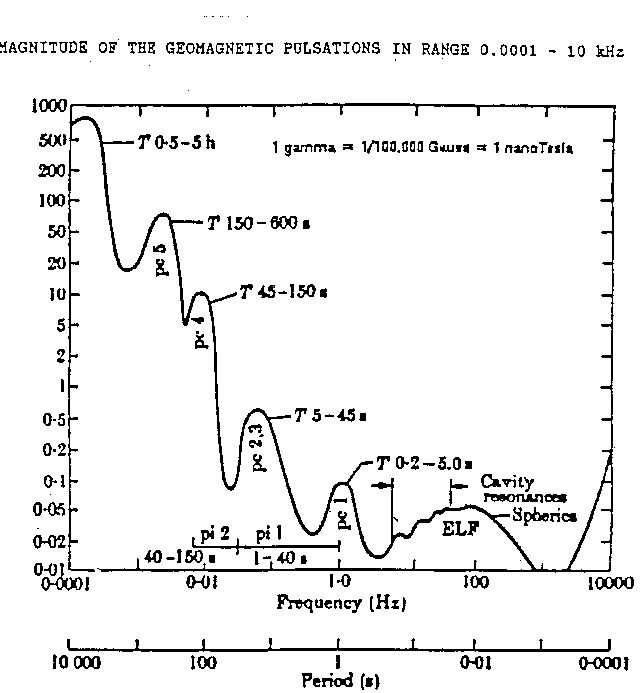
FIGURE 4 : MAGNETOSPHERIC RESONANCE - POSSIBLE DRIVING FREQUENCIES FOR BIOLOGICAL SYSTEMS (source Biddeford Figure 6)
Now, the interesting thing about resonating systems is that they tend to entrain each other. For instance, two connected vibrating strings will each attempt to pull the other into their own particular favoured resonance frequency. What often appears to happen in natural systems is that external resonances found in the environment create a tendency for smaller systems (e.g. a human being) to resonate to that frequency (e.g. see Brain Web). This brings up all sorts of esoteric issues related to presence and connectedness to the environment. Physically, it means that the apparent chaos within the arterial system is probably not truly chaotic, but rather chaos moderated by a set of external patterns, to which it finds the closest harmonic posisble. For an extremely interesting discussion of natural resonant patterns, see Ray Tomes.
It is possible that the long-period vascular rhythms entrain or are entrained by other rhythms, resonances and beats in the body. This may include cellular metabolic frequencies. There is a coherence in natural systems which is necessary for life - indeed, it could be argued that life is defined by that coherence. Certainly, consciousness requires coherence, and altered meditative states appear to encourage greater coherence.
The chaotic arterial resonance model has other less technical advantages. It provides a possible physiological link between the CSR and the greater circulation described in Taoist medicine, and also agrees with the Chinese assertion that "Chi follows Blood". There is no longer a need for a pressure or strain gauge within the sagittal suture, although, considering how many parallel systems operate in the body, I certainly would not discount the possibility of their presence. Instead, CSF flow is regulated by pressure differentials and local flow resistances. I have presented a more complex mechanism of CSF flow; dependent on hydrostatic, thermal, chemical and electrical differentials between the CSF and vascular systems, possibly regulated as much by coupled electro-osmotic effects as by the conventionally measured hydrostatic differentials.
However, the essential nature of the physiological CSR remains simple - rhythmic squeezing of the CSF due to spontaneous arterial motility. This may be augumented by other entrained or entraining cellular periodicities. Flow of CSF continues in the background, regardless of the CSR. This to me is a far more comfortable mechanism - I have never been very keen on the idea that the CSF stops production during a stillpoint, and with chaotic arterial resonance, the CSF flows on unabated. This is intuitively correct, since some stillpoints last half and hour or more, and it feels important that the flow of neurotransmitters through the CSS and out into the bloodstream is maintained.
The possibility of arterial squeezing in the spine as a mechanism for the vertical movement of CSF would also tie in with the ability of the rhythm to be bidirectional, to change resonant frequency, and to be chaotic or even palpably "still". Any frequency longer than 1 cycle per 5 minutes or faster than about 20Hz would be palpably "still". The "stillpoint" is not necessarily a true stillness, because of this narrow window of palpatory perception. Indeed, its nature (a powerful feeling of charged atmosphere in the room, accompanied by alpha state heightened awareness) subjectively suggests to me a high frequency wave on a very low frequency carrier.
As the arterial resonance changes - so does the direction, amplitude, number of nodes, and frequency of the CSR. Finally, the phenomenon of arterial resonance would be a strong contender for the phenomenon of the "therapeutic pulse". The model even provides a glimmer of how these phenomena come about as a result of treatment. I don't think arterial chaotic resonance is the full story, but I do think it accounts for a substantial chunk of the physiology related to CST, CSR's, the behaviour of the CSS and healing in general.
Incidentally, recent research also goes some way further towards answering my original question about cardiac pulses being felt (or not) in the CSR. Arterioles have a negative pressure-diameter relationship slope - i.e. they tighten as the pressure increases. This very interesting phenomenon suggests that the arteries might pump the blood (rather than the heart). A background 10 second pulse (i.e. 0.1Hz or 6cpm - surprise, surprise ... just about the standard first level CSR) appears to originate from the sympathetic system. Typical frequencies feeding into the heart sinus node (in a feedback loop to the CNS via the baroreceptor network) recorded by HeartMath are
This Sympathetic signal may be the driving frequency which maintains the resonant arterial pattern. It would be very useful to simultaneously measure CSR along with pulse during the HeartMath experiments - this would give an indication as to whether the 0.1Hz sympathetic input is a driving beat, or is driven by (i.e. occurs at the same frequency as) the CSR. It is interesting that pathological nerve loss is associated with a CSR of about 20 to 30cpm, which falls in the parasympathetic frequency range. My understanding of the Autonomic Nervous System is insufficient to be able to say whether this is "just" a coincidence or a meaningful coincidence. However, this brings us around to two further considerations
It may be that there is a fundamental tide in the body which causes the (approximately) 10 second rhythm in the sympathetic output, which in turn causes rhythms with peroids in excess of 10 seconds to appear in the arterial system. The various phenomena found in craniosacral work are far more varied than a single 10-second periodicity. I therefore feel that a chaotic resonant frequency source - such as found in the arterial system - is the physiological phenomena we are actually feeling when we work craniosacrally.
Ultimately, all the systems of the body are complex feedback loops, and so it may be a rather pointless question to ask what causes what. If a cranial-type rhythm stimulates the sympathetic system to produce a rhythm which regulates chaotic resonance in the arterial system, which then superposes a broad spectrum pattern to produce a beat which feeds back into electromagnetic resonances in the cells fo the body, which entrains the central nervous system, which causes a Cranial type rhythm, (etc ad nauseam), then which is the chicken and which is the egg? My sense is that all these mechanisms (and more) are constantly interweaving and regulating each other, so the concept of a single "causative factor" may be in practice difficult to pin down... An understanding of the possible entrainment pathways - and the relative strengths of their input into the total system in different circumstances may lead to more focussed and effective treatment practices.
The heart has been called a pump ever since its dissection in the 17th Century. At that time, the only pump available as a model was the positive displacement pump used for mine drainage, fire engines, and blacksmiths bellows. Today there are quite different pumps to use as possible models for the Heart. The Ram Pump requires no motor or active pumping by the "pump" - instead, it acts as a flow regulator and clapper valve, and so transmits a pulse of energy back into the water.
Consider two sets of pipes resonating at different frequencies, joined together in a chamber with valves. It doesn't seem too far fetched to imagine that the pulse of the heart is actually a response to converging resonant beats in the arteries and veins. We now have another chicken and egg situation. Does the heart pump the blood, or does the blood pump the heart? Remember that arterioles contract as blood pressure rises!
This further begs the question of exactly what is the ECG? If the blood pumps the heart, then what is a huge electrical surge doing in our bodies every second? I would like to make the flimsy and totally unsupported proposal that the output of the ECG is actually one of the major functions of the heart - and its function in blood flow is more as a regulator valve. This would explain the very early occurence of blood circulation during embryonic growth. The heart may be an electrical generator - providing a timed electrical charge to every cell in the body. The electricity of life.
It could be that making the CSS more mobile reduces back-pressure on the arterial chaotic resonance, and so makes the chaotic system more resilient. This may be one of the major physiological mechanisms which underpin the effectiveness of CST.
You could (as in the case of a CV4) create a node at one point, and allow a resonant pattern to develop around that point of stillness. This may explain the general principle that effective treatments are often at the opposite end of the body from the apparent problem - local stillness creates a greater resonance at a distance.
And there are probably lots more implications besides. I hope you have fun with this model.
1. Spontaneous diameter oscillations of the radial artery in
humans.
Hayoz D, Tardy Y, Rutschmann B, Mignot JP, Achakri H, Feihl F, Meister JJ,
Waeber B, Brunner HR
Am J Physiol 1993 Jun 264:6 Pt 2 H2080-4
(Variations in arterial diameter of the Radial Artery, average 80 microns,
period 45-70 seconds - about 1cpm - with NO corresponding change in BP)
2. A theoretical investigation of low frequency diameter oscillations
of muscular arteries
Achakri H, Rachev A, Stergiopulos N, Meister JJ
Ann Biomed Eng 1994 May-Jun 22:3 253-63
(theoretical study showed that under certain conditions, including the fact
that arterioles have increased diameter with lower pressure, their behaviour
becomes semi-chaotic, and a periodic beat occurs in critically branched systems
- i.e. there is a natural resonance of the vascular system)
3. Relationship between low-frequency oscillations of blood pressure and
changes in arterial diameter.
Siché JP, De Gaudemaris R, Riachi M, Mallion JM
J Hypertens Suppl 1992 Aug 10:6 S45-8
(periodic changes in arterial compliance - 15 to 250 second cycles or 4 to
0.4cpm were measured)
4. Flow-diameter phase shift. A potential indicator of conduit artery
function
Hayoz D, Bernardi L, Noll G, Weber R, Porret CA, Passino C, Wenzel R,
Stergiopulos N
Hypertension 1995 Jul 26:1 20-5
(cycles of >50seconds or 1cpm showed that blood flow changed an average
of 20 seconds in advance of diameter changes, implying a frequency of 80
seconds per cycle - driven resonance being typically ¼ cycle out
of phase)
5. Theoretical analysis of complex oscillations in multibranched microvascular
networks
Ursino M, Cavalcanti S, Bertuglia S, Colantuoni A
Microvasc Res 1996 Mar 51:2 229-49
(vascular systems create chaotic resonance frequencies, and small changes
in smooth muscle tension have a large impact on frequencies. Different
frequencies cause flow pertubations which change the proportional routing
of blood at junctions)
6. Heart rate response to hemorrhage-induced 0.05-Hz oscillations in arterial
pressure in conscious dogs
Madwed JB, Cohen RJ
Am J Physiol 1991 Apr 260:4 Pt 2 H1248-53
(loss of blood causes a 20-second - 3cpm - cyclic pulse in blood pressure)
7. Rhythmical fluctuations of the intracerebral microcirculation studied
in pigs
Kirkeby OJ, Rise IR, Risöe C
Int J Microcirc Clin Exp 1995 Nov-Dec 15:6 316-24
(not pretty reading, but rythmic changes in blood flow - with no associated
changes in csf or arterial pressure! - were noted, period approx 13 to 30
seconds - 4.5 to 2 cpm)
8. Investigating the origin of cyclic changes in limb volume using
mercury-in-silastic strain gauge plethysmography in man
Christ F, Raithel P, Gartside IB, Gamble J, Peter K, Messmer K
J Physiol (Lond) 1995 Aug 15 487 ( Pt 1) 259-72
(unilateral!!! dilation and contraction of the lower leg - volume change
less than 0.02% - at a frequency of 8-30 seconds - 8 to 2 cpm - observed,
with no correlation between breath, arterial BP or venous BP - attributed
to vasomotion)
9. Variations of rhythmic diameter changes at the arterial microvascular
bifurcations
Colantuoni A, Bertuglia S, Intaglietta M
Pflugers Arch 1985 Mar 403:3 289-95
ABSTRACT The variation of the pattern of the rhythmic diameter changes, ...
was studied sequentially along the branching network of the arterial vessels,
from A1 small arteries (70-100 micron diameter) to A4 terminal arterioles
(less than 15 micron diameter). Contraction and dilation waveforms were
characterized at all subsequent levels of bifurcation. It was found that
the frequency of vasomotion changes abruptly at the branching points,
systematically increasing in the downstream direction. The power spectrum
showed that the frequencies, which appear to originate at the bifurcations
and have maximum amplitude at these points, are also found in the upstream
waveforms. The downstream propagation of contractions and dilations causes
superposition of waves. Thus the pattern of vasomotion is the composite effect
of signals that originate at various branching points and spread downstream
and upstream in the microvasculature. ... This time dependent phenomenon
affects deeply the microvascular blood flow.
10.
Cardiac
Coherence: A New Noninvasive Measure of Autonomic Nervous System
Order
William A. Tiller, Rollin McCraty and Mike Atkinson
Published in Alternative Therapies in Health and Medicine,1996;2(1):52-65
(Shows 0.1Hz (6cpm) heartbeat resonance, and ECG's for calm and emotionally
charged states)
11. Netter, Frank H. (1996) Atlas of Human Anatomy. Publ CIBA-GEIGY Corporation.
12. Cade, M and Coxhead, N. (1996) The awakened mind : Biofeedback and the development of higher states of awareness. Publ Element Books
12Zimmerman, J. (1990) The laying on of hands and therapeutic touch : a testable theory
Journal of the Bio-Electromagnetics Institute 2 (pp9-17)
12Fenerstein, George (19??) Sacred paths (p153)